
Maxalt
Maxalt 10mg
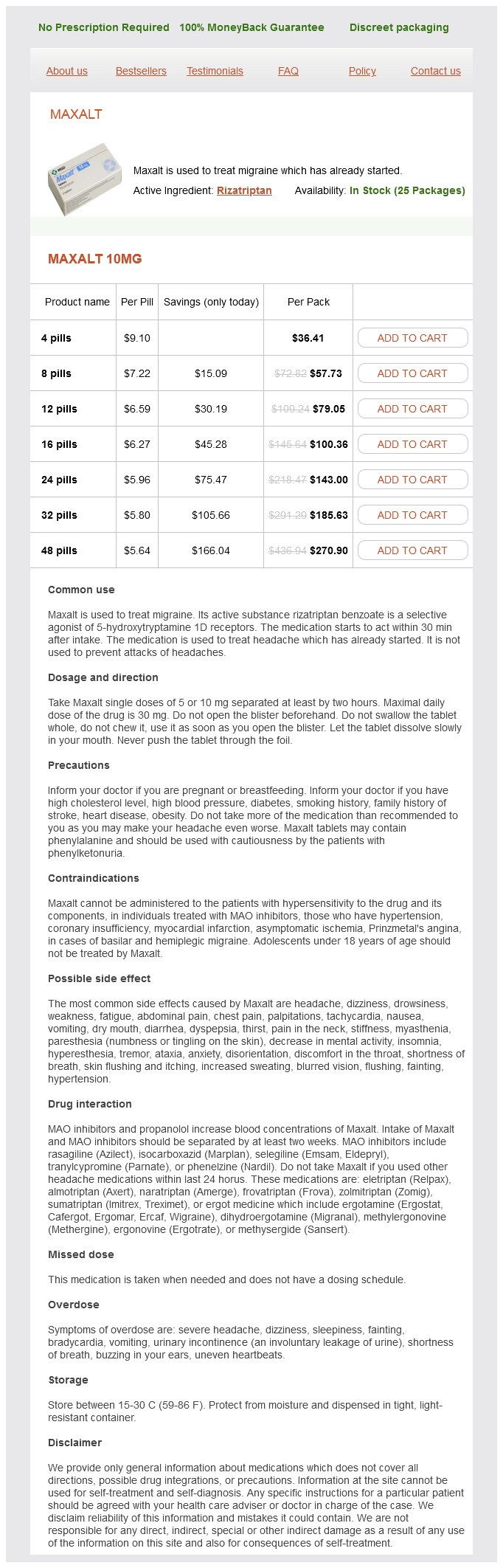
- 4 pills - $36.41
- 8 pills - $57.73
- 12 pills - $79.05
- 16 pills - $100.36
- 24 pills - $143.00
- 32 pills - $185.63
- 48 pills - $270.90
Due to improvements in surgical technique chronic pain treatment guidelines 2013 maxalt 10 mg purchase on-line, donor-recipient matching, graft surveillance, and immunosuppression, pancreas transplant graft survival has improved and now matches graft survival rates of kidney and liver transplant. Despite these improvements, the rates of pancreas transplants in the United States peaked in the early 2000s and declined steadily thereafter. This represented a 7% increase in total pancreas transplants from the year prior, the first yearly increase in more than 10 years. Additionally, all pancreas transplant candidates are placed on a single waitlist and given equal priority to pancreas donors, regardless of the type of pancreas transplant they are to receive. Rare indications for pancreas transplant include select cases of type 2 diabetes mellitus, chronic pancreatitis that has developed endocrine deficiency, cystic fibrosis with endocrine deficiency, and prior total pancreatectomy. Previously pancreas transplant was reserved for younger patients, traditionally under age 40. Recent single-center studies have demonstrated similar results in pancreas transplant recipients over age 50 compared to younger patients. Patients with diabetes have a high cumulative prevalence of blindness (16%), renal failure (22%), lower extremity amputation (12%), myocardial infarction (21%), and stroke (10%). Patients with type 1 diabetes are prone to large fluctuations in blood glucose levels. Hypoglycemic episodes contribute to acute morbidity and mortality in diabetic patients. Hypoglycemia unawareness in particular can have a marked impact on quality of life and is a frequent indication for pancreas transplant. Pancreas transplant centers pursue a comprehensive, multidisciplinary evaluation and selection process before listing candidates. The evaluation should address the organ systems most affected by long-standing diabetes, including the cardiovascular, renal, and neurologic systems. Previously, patients considered for pancreas transplantation were younger than 50 years and had a lower risk for the cardiac and vascular sequelae of diabetes. Blood glucose measurements should be assessed closely before surgery and recent insulin administration should be noted. Most patients will have a preoperative variable-rate intravenous infusion of insulin with maintenance glucose during a period of fasting. Type 2 diabetes mellitus results from peripheral resistance to the effects of insulin. Both diseases produce chronic increases of blood glucose concentrations resulting in the multiorgan manifestations of diabetes. The chronic complications of diabetes that have the greatest effect on patient morbidity and survival are those that affect the cardiovascular system. Serial trends in heart rates and arterial blood pressures in hospitalized patients should be assessed, as most patients will have a history of hypertension requiring multiple medications, especially patients with renal failure.