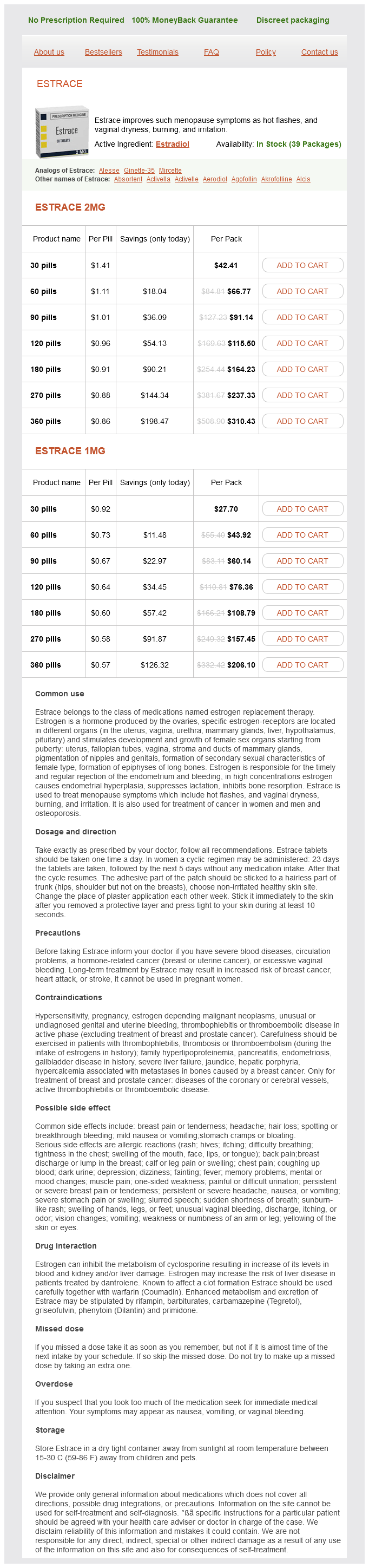
Estrace
Estrace 2mg
- 30 pills - $42.41
- 60 pills - $66.77
- 90 pills - $91.14
- 120 pills - $115.50
- 180 pills - $164.23
- 270 pills - $237.33
- 360 pills - $310.43
Estrace 1mg
- 30 pills - $27.70
- 60 pills - $43.92
- 90 pills - $60.14
- 120 pills - $76.36
- 180 pills - $108.79
- 270 pills - $157.45
- 360 pills - $206.10
This assessment was strengthened by the absence of significant renal haemodynamic effect reported in other types of anaemia breast cancer 9 lymph nodes estrace 2 mg order amex, such as iron deficiency anaemia (Bradley et al. The role of these mediators has remained under investigation for more than a decade with no comprehensive view to date. The prevalence of proteinuria within the nephrotic range is low (< 4%) (Bakir et al. The identification of relevant determinants responsible for albuminuria is still under debate. Micro- and macroalbuminuria may be mediated by different factors corresponding to selective and non-selective proteinuria. Conversely, macroalbuminuria corresponds to the presence of non-selective proteinuria assessed by an increased dextran permeability clearance with an incremental increase in the pore radius (Guasch et al. Medulla vasa recta rarefaction and maximally hypertrophied glomeruli with or without focal sclerosis are two striking features detected in most cases. Vascular lesions Haemoglobin polymerization is responsible for sickled red blood cell occlusion of blood flow in vasa recta resulting to typical medullary and papillary necrosis in 1536% of cases (McCall et al. Glomerular capillary obliteration is also described at a later stage (Bhathena and Sondheimer, 1991) (see below). Glomerular lesions Glomerular hyperfiltration is characterized by a distinctive morphological pattern with glomerular enlargement, compared to control subjects (Bernstein and Whitten, 1960; Pitcock et al. In adult patients, glomerular size is increased by > 50% compared to controls (Elfenbein et al. In older patients with glomerular involvement, progressive ischaemia and fibrosis lead to glomerulosclerosis. It is thus tempting to speculate that glomerular enlargement with capillaries distended by sickled erythrocytes could both explain hyperfiltration at early stage of the disease and the increased occurrence of a variety of immune and non-immune mediated glomerular lesions. Tubulointerstitial lesions Abundant haemosiderin granules in proximal tubular epithelial cells are reported in most biopsies (Bhathena and Sondheimer, 1991; Maigne et al. Focal necrosis, oedema, and extensive areas of fibrosis are reported in the papilla (Saborio and Scheinman, 1999). Renal dysfunction is reported to the stimulation of the local reninangiotensin system is probably at play with little impact on systemic blood pressure, conversely to other nephropathies (including diabetes at the time of hyperfiltration). Indeed, despite a higher diastolic blood pressure in albuminuric compared to non-albuminuric patients (Bolarinwa et al. In this regard, haemosiderin deposits should draw our attention as they may indicate an imbalance skewing to a pro-oxidant state within tubules (and possibly endothelial cells) which may explain tubular lesions. Renal biopsy indication Percutaneous renal biopsy can be performed when indicated after a complete coagulation profile and thus sometimes requires a red blood cell transfusion or exchange as a preconditioning. Of note, a few acute nephrotic syndromes worsening a pre-existing albuminuria were reported to be linked to parvovirus B19 infections (Wierenga et al.
Isolated tubular interstitial nephritis in a patient with systemic lupus erythematosus Nefrologia pregnancy leggings buy discount estrace 1 mg, 29(5), 5012. Tubulointerstitial changes as a major determinant in the progression of renal damage. Influence of clinical variables, biopsy, and treatment on the outcome in 150 patients with lupus nephritis seen at a single center. Isolated sarcoid granulomatous interstitial nephritis: review of five cases at one center. Predominant tubulointerstitial nephritis in a patient with systemic lupus erythematosus: phenotype of infiltrating cells. Repeat renal biopsy in children with severe idiopathic tubulointerstitial nephritis. Autoantibodies against monomeric C-reactive protein in sera from patients with lupus nephritis are associated with disease activity and renal tubulointerstitial lesions. Repeat renal biopsy in a girl with tubulointerstitial nephritis and uveitis syndrome. Osteomalacia revealing celiac disease and primary biliary cirrhosis-related Fanconi syndrome in a patient with systemic sclerosis. Isolated sarcoid granulomatous interstitial nephritis responding to infliximab therapy. Rituximab therapy for refractory biliary strictures in immunoglobulin G4-associated cholangitis. A 58-year-old man with sarcoidosis complicated by focal crescentic glomerulonephritis. Sarcoid tubulo-interstitial nephritis: long-term outcome and response to corticosteroid therapy. Mortality of intrathoracic sarcoidosis in referral vs population-based settings: influence of stage, ethnicity, and corticosteroid therapy. Membranous nephropathy associated with IgG4-related systemic disease and without autoimmune pancreatitis. Tubulointerstitial nephritis and uveitis syndrome: a case with an autoimmune reactivity against retinal and renal antigens. Distinctive pulmonary histopathology with increased IgG4-positive plasma cells in patients with autoimmune pancreatitis: report of 6 and 12 cases with similar histopathology. Renal impairment in sarcoidosis: granulomatous nephritis as an isolated cause (two case reports and review of the literature). Tubulointerstitial nephritis and uveitis syndrome with autoantibody directed to renal tubular cells. Inflammatory pseudotumour (inflammatory myofibroblastic tumour) of the pancreas: a report of six cases associated with obliterative phlebitis.
Sclera Acquired u (B) Scleritis is the most common eye involvement in antineutrophil cytoplasmic antibody-associated vasculitides menstrual man cheap estrace 1 mg with amex. Granulomatosis with polyangiitis (Wegener granulomatosis) is the most common cause of scleritis in patients with systemic vasculitides. Nephrogenic systemic fibrosis or nephrogenic systemic dermopathy which occurs not exclusively in dialysis patients, but in renal failure patients after exposure to gadolinium magnetic resonance imaging contrast agents: asymptomatic scleral involvement can be seen in as many as 75% of cases. Patients present with telangiectasia mimicking conjunctivitis and later yellow scleral plaques can be seen (Knopp and Cowper, 2008). They are similar to changes caused by systemic drugs such as amiodarone or chloroquine, but can be distinguished by appearance and history. Further lesions of the eye lids, iris nodules, recurring hyphaema and a subcapsular cataract can be seen (Sodi et al. The renal pathology reveals accumulation of a degradation product of glycosphingolipid mainly in podocytes and tubulus cells. Renal pathological changes such as tubulointerstitial fibrosis and glomerular damage are closely associated with the residual alpha-Gal A activity. The prognosis for this form depends on the extent to which the disease affects renal function: the accumulation of abnormal lipoproteins in the kidneys may lead to renal insufficiency. Variable renal abnormalities such as unilateral absence, unilateral or bilateral hypoplasia, and cystic dysplasia have been reported. Other systemic manifestations include pre-auricular skin tags and/or pits (which are probably the most consistent feature), congenital heart defect, and usually low-normal intelligence. A wide range of additional abnormalities include posterior embryotoxon, megalocornea, iris hypoplasia, cataract, abnormal lens shape, posterior lenticonus, persistent fetal vasculature, retinal detachment, variable axial lengths, and glaucoma. Nail-patella syndrome: a cloverleaf dark pigmentation of the central area of the iris with scalloped iris collarette (Lester sign of the iris) is a peculiar finding. Strabismus, keratoconus, microcornea, sclerocornea, microphakia, and cataracts have been described (Meyrier et al. Treatment In case of vision disturbing band keratopathy, one would be abrading the calcium deposits after applying chelating agents. In rare cases, corneal dystrophies will require a corneal transplant to rehabilitate the vision, as the underlying disease persists the transplant may become affected over time. In recurrent corneal erosion, applying artificial tears and bandage contact lenses is helpful. Treatment of the corneal deposits in cystinosis with cysteamine eye drops has shown promise (Gahl et al. Ocular symptoms (redness, pain, photophobia) often precede renal disease (Mackensen and Billing, 2009). In addition, alterations of the cornea and angle malformations can occur which lead to glaucoma, cataract formation, and retinal malformation (Lee et al. Treatment Aniridia can be treated by surgical methods which try to rebuild the iris. Other approaches include tattooing the cornea or contact lenses with an iris imprint.
Figwort (Lesser Celandine). Estrace.
- Are there safety concerns?
- How does Lesser Celandine work?
- Dosing considerations for Lesser Celandine.
- Bleeding wounds and gums, swollen joints, warts, scratches, scurvy, and hemorrhoids.
- What is Lesser Celandine?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96547
Syndromes
- Infection with the bacteria that cause Lyme disease
- White or clay-colored stools
- Disfigurement of the face
- After you have done the stimulation, sit in a normal posture for a bowel movement. If you are able to walk, sit on the toilet or bedside commode. If you are confined to the bed, use a bedpan. Get into as close to a sitting position as possible, or use a left side lying position if you are unable to sit.
- High blood pressure
- Follow safe sex practices. If you are diagnosed with chlamydia or another STD, all of your sexual partners need to be checked. If they are infected.
- Angina (angina pectoris) - stable
Usage: q._h.
Additional information: