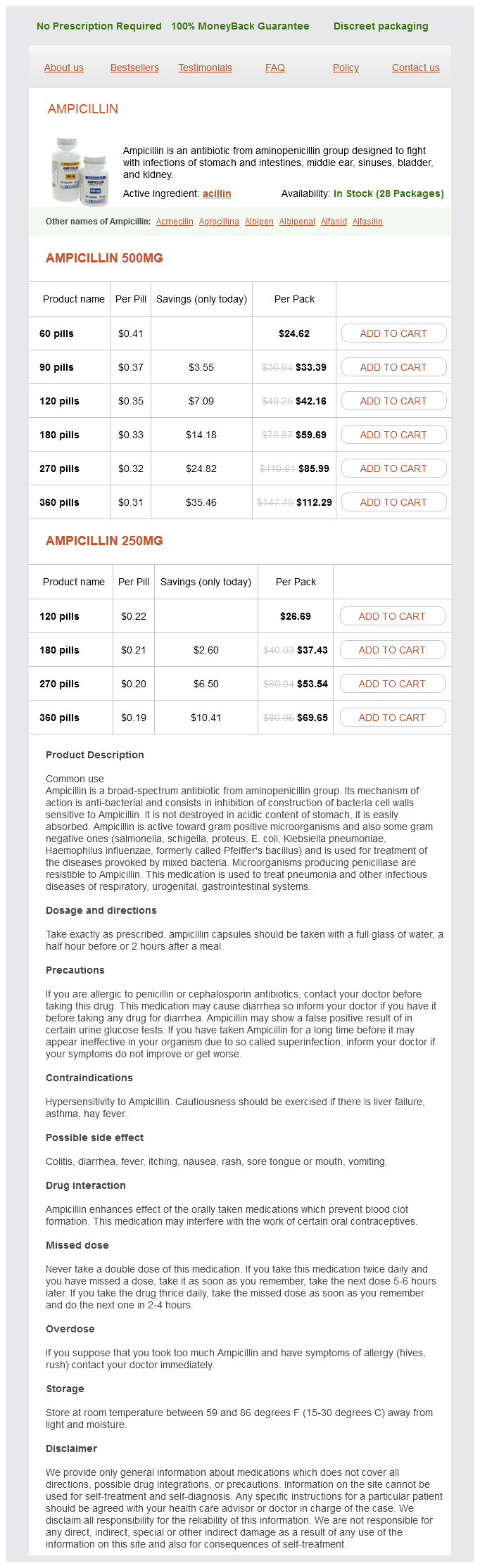
Ampicillin
Ampicillin 500mg
- 60 pills - $24.62
- 90 pills - $33.39
- 120 pills - $42.16
- 180 pills - $59.69
- 270 pills - $85.99
- 360 pills - $112.29
Ampicillin 250mg
- 120 pills - $26.69
- 180 pills - $37.43
- 270 pills - $53.54
- 360 pills - $69.65
There is death of the trabecular bone and bone marrow antibiotics joke safe ampicillin 500 mg, followed by collapse of the bony architecture. Later on, after the femoral head bone has collapsed, the signs are similar to those of an arthritic hip. The diagnosis is confirmed in later cases by plain radiographs as these show the collapse of the femoral head and narrowing of the joint space. Aseptic Loosening of the Hip Some patients have a satisfactory outcome of their hip replacement for several years before progressively increasing pain develops in the groin or thigh. There is an associated stiffness, an inability to bear weight and a progressive limitation of the range of motion. Examination involves flexing the hip and the knee to 90° and applying axial compression or traction to the femur. This often produces pain as the femoral component of the prosthesis pistons or subsides within the femur. A plain radiograph will show a defined sclerotic line around the loose stem and, in advanced cases, migration of the prosthetic components. Meralgia Paraesthetica this is a compressive neuropathy of the lateral femoral cutaneous nerve of the thigh when it becomes entrapped under the inguinal ligament or occasionally through the fascia lata. This nerve is purely sensory, resulting in an area of hyperaesthesia and tingling over the lateral aspect of the thigh. This is worse on standing and walking but is relieved by sitting as flexion of the hip shortens the course of the nerve. This affords particular advantages in allowing a good range of movement and reducing the frictional torque within the hip. The direction of the dislocation is governed by the alignment of the acetabular and femoral components, as well as the surgical approach used. With the commonly used lateral surgical approach, the risk of dislocation is greatest when the hip is flexed and adducted. The patient complains of sudden severe pain in the hip and feels the hip popping out of the socket. In a posterior dislocation the leg is short and internally rotated, while in an anterior dislocation it is short and externally rotated. Trochanteric Bursitis this is inflammation of the trochanteric bursa that occurs mainly after increased physical activity. Palpation over the greater trochanter causes pain, as may getting the patient to abduct their leg against resistance. In extensive cases, there is a progressive limitation of movement as bony islands can coalesce between the femur and pelvis.
It is usually asymptomatic in the initial stages and progresses to loss of vision in the later stages antibiotics cephalexin ampicillin 500 mg online. Patients frequently present with headaches or frequent change of prescriptions for spectacles. The optic disc shows progressively increased cupping in its initial stage that can only be picked up on routine ophthalmic examination. It is therefore recommended that individuals with no apparent risk of glaucoma undergo a routine check-up every 5 years, and those who are at risk have a check-up every year. Strabismus the ocular movements are usually well coordinated, keeping the eyes aligned. A concomitant or non-paralytic squint is one in which the angle of deviation does not change irrespective of the fixation taken by a normal or squinting eye, and is the same in any direction of gaze. There are various causes of concomitant squint, including hereditary, ametropic, anisometropic and amblyopic. Head injury, thyroid gland disease and myasthenia gravis are among the common causes of a paralytic squint. The Pupil Neurological causes Abnormal pupillary responses may be a sign of a central nervous system disease but may also result from disease of the optic and oculomotor nerves, and from the effects of disease and drugs on the eye itself. An Argyll Robertson pupil is a small pupil that is non-reactive to light but reacts to convergence. A HolmesAdie pupil is a large pupil that has a poor or abnormal reaction to light or near reflex but may slowly dilate in a darkened room or with mydriatics. The cause is unknown but it results from myotonia, occurring in association with depressed tendon reflexes and anhidrosis of the limbs. It is characterized by ipsilateral miosis (pupillary constriction), ptosis (drooping of the eyelid), vasodilatation (flushing of the face, with increased temperature) and anhidrosis of the face, all occurring on the same side as the underlying lesion. Eye signs may occur in isolation with interruption of the intracranial sympathetic plexus around the carotid artery. The pupil is poorly reactive in both the direct (light in the affected eye) and consensual (light in the other eye) light reflexes. A Marcus Gunn pupil has a relative afferent pupillary defect, that is, an absent direct pupillary reflex but a good consensual reflex on the affected side. The unaffected eye has a diminished response to stimulation of the affected eye by light. Non-neurological causes Abnormalities of the shape of the pupil may result from colobomas congenital notching of the iris or be secondary to globe injury or glaucoma. Drug-induced pupillary constriction occurs with miotic eye drops, such as pilocarpine, and opiates. Drug-induced pupillary dilatation occurs with anticholinergic drugs, including mydriatic eye drops, such as atropine, and cocaine. Nystagmus Nystagmus is rhythmic, involuntary oscillations of the eye and may be congenital, voluntary or physiological. As a localizing sign, it is most often described in relation to vestibular and cerebellopontine angle disease.
Over the years viral load order 250 mg ampicillin, a series of terms have been used and abandoned, including fibroadenosis, chronic mastitis, cystic mastopathy and benign mammary dysplasia. The aetiology is poorly understood but is likely to involve the action of cyclical circulating hormone levels on breast tissue. The most common site for lumps and nodularity is the upper outer quadrant and axillary tail (and unfortunately this is also the most common site of breast cancer because this quadrant has the largest volume of breast tissue). The stage is a strong predictor of the prognosis and helps to determine the treatment; therefore precise staging is essential, and the reader is advised to consult an up-to-date staging manual. Malignant breast lumps tend to enlarge progressively and generally do not change with the menstrual cycle. Nipple discharge if present is usually serous or serosanguinous, and the location of the duct may help to predict the quadrant in which the underlying tumour is found. A delay in diagnosis is particularly common in young women (in whom the diagnosis may not be considered), during pregnancy or with rapidly growing tumours, which may simulate infection. The clinician must thus maintain a high index of suspicion for this common malignancy. The diagnosis can be established by the aspiration of green or straw-coloured fluid and the disappearance of the mass, or by ultrasound (see below). Fibroadenomas Fibroadenomas are benign tumours of the breast that are common in women in their late teens to their early 30s. Most fibroadenomas grow to 12 cm in diameter, and their size can fluctuate due to the influence of hormones during the menstrual cycle. These benign masses usually present as a hard, painless lump that is freely mobile on palpation. There is no clear consensus on whether a fibroadenoma should be surgically removed. If the triple test is consistent with a fibroadenoma, the lesion can be managed conservatively with a follow-up examination in 6 months. There is often a characteristic oil cyst (a collection of lipids surrounded by a membrane) on mammography in the area of trauma, leading to the diagnosis of fat necrosis; however, the area of trauma may reveal fibrosis and calcifications that may mimic malignancy on mammography. If the patient does not recall trauma to the breast or imaging does not reveal an oil cyst, the area of concern should undergo a core or excisional biopsy to obtain a histological diagnosis. Galactoceles these are milk-filled fluid collections most commonly seen during lactation or after the cessation of lactation. Abscesses A subareolar abscess is often a recurring condition that is secondary to disease of the subareolar ducts. If the infection is early in its course and there is no underlying abscess cavity (induration with no fluctuance on palpation), a course of oral antibiotics should be prescribed.
Colle du Japon (Agar). Ampicillin.
- What is Agar?
- How does Agar work?
- Dosing considerations for Agar.
- Are there safety concerns?
- Are there any interactions with medications?
- Constipation, diabetes, weight loss, and obesity.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96124
Syndromes
- Diarrhea for more than 2 days or vomiting for more than 12 hours in an infant or child -- call right away
- National Digestive Diseases Information Clearinghouse - http://digestive.niddk.nih.gov/ddiseases/pubs/fecalincontinence
- Voice box (larynx)
- When did this movement begin?
- You will usually be asked not to drink or eat anything for 6 to 12 hours before the procedure.
- Infection (heterotaxy with no spleen)
- Where to buy diabetes supplies and how to store them
- Obesity
Usage: q.d.
Additional information: